
Scarlet Fever: A Deadly History and How it Prevails

Why did scarlet fever used to be such a dangerous disease, and why (although the burden of disease is far less than in years past) do outbreaks continue to occur, even after the development of penicillin?
History of Scarlet Fever
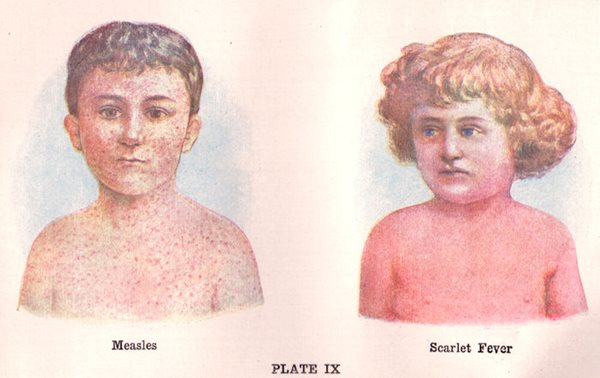
The first notable description of what might have been scarlet fever was documented by the Sicilian physician Giovanni Filippo Ingrassia in 1553. Ingrassia, who was well-known for his anatomical studies and contributions to public health, called the disease "rossalia” and described the patient as having "numerous spots, large and small, fiery and red, of universal distribution so that the whole body appeared to be on fire."
Throughout the remainder of the 1500s and most of the 1600s, various scientists and physicians around the world added elements to the definition of the disease, further distinguishing it from other rash-causing illnesses like measles. For example, German physicians described an outbreak of a similar disease to "rossalia” in 1564. They termed it "scarlatina anginosa," noting that it was particularly fatal to infants and that patients presented with a sore throat, violent fever, vomiting and swelling of the parotid glands, in addition to a rash.
In 1578, the French nobleman Jean Cottyar of Poitiers was credited with providing the first definitive description of the disease by tying all previous descriptive elements together and adding a few—namely that purpura appeared in patients on the second or third day, accompanied by a sore throat.
While epidemics of scarlet fever raged through Europe and North America through the 17th and 18th centuries, it was not until the 1920s that the significance of the patient’s sore throat would be fully realized. In 1924, American bacteriologists Gladys and George Dick demonstrated that the cause of scarlet fever was the beta-hemolytic organism Streptococcus pyogenes (S. pyogenes, also called group A streptococci) and that a toxin produced by the organism could cause this severe downstream disease, or even progress to the development of rheumatic fever later in life.

Current Outbreaks
Since September 2022, there has been a significant outbreak of scarlet fever in children in Europe, and more recently, there have been documented increases in cases in the U.S. This outbreak has been unique in that it first appeared out of sync with typical seasonality and has come with higher mortality rates than normal. For example, the outbreak began in late summer and has killed 13 children under 15 in England since September. Between September and November 2022, public health agencies in England reported 4,622 cases of scarlet fever, a value significantly higher than the previous 5-year average of 1,294.
While the reasons for the increase in scarlet fever are unclear, hypotheses include macrolide resistance, weakened herd immunity, environmental factors and the absence of a vaccine for the bacteria that cause the disease (group A strep) Additionally, rates of scarlet fever increase with the start of the school year and as winter approaches. This may be attributed to the absence of immunity or the greater risk of crowding indoors during colder months.
The World Health Organization (WHO) has stated that the observed increase in cases may coincide with the early start of the respiratory season and the high incidence of circulating respiratory viruses. Additionally, children may be more significantly impacted due to decreased immunity stimulated by group A streptococcal infections during the COVID-19 pandemic years. However, this theory is unsubstantiated at this time.
Importantly, antimicrobial susceptibility test results from routine laboratory surveillance in England did not demonstrate any increased antibiotic resistance among S. pyogenes organisms, indicating that drug resistance is not responsible for increased virulence or spread of the organism in the current outbreak.
Expanded surveillance and research are needed to understand these outbreaks, but the pathogenesis and epidemiology of the disease provide additional context clues.
Who Is Susceptible to Scarlet Fever?
Scarlet fever can occur in people of all ages, however, the disease occurs most often in school-age and adolescent children, due to the ease of transmissibility in classrooms and daycares and lack of immunity to protective antigens of group A strep. While group A strep is not responsible for all cases of pharyngitis (strep throat) in children, it is believed to be the cause of 15-30% of all pharyngitis cases in children 5-15 years of age.
Why Do Some People Get Scarlet Fever and Others Don’t?
Not all patients who acquire group A strep pharyngitis will develop invasive streptococcal disease. In fact, a significant proportion of school-aged children carry S. pyogenes in their upper respiratory tract without any signs or symptoms of infection. The extent to which a person will become ill due to a group A strep infection relies on the production of a type of exotoxin called bacterial superantigens (SAgs) and how the patient’s body responds to them.
In some patients, the release of group A Strep bacterial superantigens induces an immune response where uncontrollable cytokines are released from the patient’s T-cells and antigen-presenting cells. This dramatic immune response (otherwise known as a "cytokine storm”) is believed to be responsible for the manifestations of toxic shock syndrome and may include symptoms such as the constriction of blood vessels, low blood pressure, low platelet count and multi-organ failure. The superantigens SpeA, SpeC and SSA have been directly associated with scarlet fever. The development of scarlet fever depends on both the strain of Group A Strep a patient gets, and how their body responds to the infection.
How Harmful Is Scarlet Fever?
Importantly, while the scarlet fever rash itself is not harmful, it is an indicator of Group A Strep disease, which can progress to invasive disease (i.e., necrotizing fasciitis or toxic shock syndrome) and be fatal, if left untreated. The Centers for Disease Control (CDC) estimates that in the last 5 years, 14,000 to 25,000 cases of invasive group A strep disease have occurred in the U.S. and that 1,500-3,000 people die yearly from these infections. It is imperative that data on the prevalence of disease are reported to public health agencies regularly and surveillance is performed at the public health level.
Diagnosing Group A Strep and Scarlet Fever

There are multiple conventional identification tests that can be used to quickly identify an organism as S. pyogenes. Any one of these tests is sufficient to identify a beta-hemolytic Streptococcus as S. pyogenes. These test methods include:
- Lancefield antigen determination: Lancefield antigen grouping serum is used to differentiate different types of Streptococci. Agglutination is observed when the organism is applied to serum with antibodies that match the presented antigen.
- Pyrrolidonyl Arylamidase (PYR) test: This test is performed using paper strips or disks that test for the presence of the enzyme pyrrolidonyl aminopeptidase, which is unique to a few gram-positive organisms, including S. pyogenes. This is a rapid colorimetric method; when the organism is applied to the disk or strip and a reagent is added, a color change will be observed.
- Bacitracin susceptibility: S. pyogenes can be differentiated from other beta-hemolytic streptococci due to its increased susceptibility to bacitracin. This test is performed by dropping a bacitracin disk on a plate with a pure culture of the organism to be tested. This test requires additional incubation, so it may be less favorable in cases where a faster turnaround time is warranted.
In addition to rapid conventional microbiology methods, S. pyogenes is readily identified using automated identification systems and MALDI-TOF. Despite its continued use to treat group A strep infections over the years, penicillin resistance has not occurred, and penicillin is still the antibiotic of choice to treat these infections. Given this, antimicrobial susceptibility testing for S. pyogenes is generally not warranted, unless a patient has a significant allergy to penicillin, and other drugs (such as macrolides) need to be tested.
WHO recommends continued surveillance and advises healthcare providers to maintain a high level of suspicion for group A strep-related diseases, as identifying and treating these infections early may prevent invasive Streptococcal disease and other serious downstream outcomes. As always, good respiratory and hand hygiene can help prevent the spread of organisms like S. pyogenes.
Watch Andrea Prinzi explain why scarlet fever used to be such a dangerous disease, and why (although the burden of disease is far less than in years past) outbreaks continue to occur, even after the development of penicillin.
The emergence of yellow fever in the United States brought death and panic, but also initiated a cascade of research and discovery. In this next article, learn how research throughout the ages led to the development of vaccines and diagnostic technology that are still commonly used today.
