This article was originally published July 31, 2020 and has been updated by the author.
The COVID-19 pandemic has created monumental imbalance to our accepted way of life, removed the illusion of host dominance and thrown a glaring spotlight on some of the tiniest members of society—viruses. During the 2020-2021 flu season, the cumulative rate of laboratory-confirmed influenza-associated hospitalizations was the lowest on record since influenza data collection began in 2005. But as time dutifully marches on, many are once again considering the risks associated with a circulating, pandemic respiratory virus clashing with the next impending flu season. In order to predict how these 2 heavy-hitting viruses might interact with one another this year, let’s take a look at what we know about each virus and the diseases they inflict. To learn more, check out our COVID-19 and Influenza Resource pages.
Virology
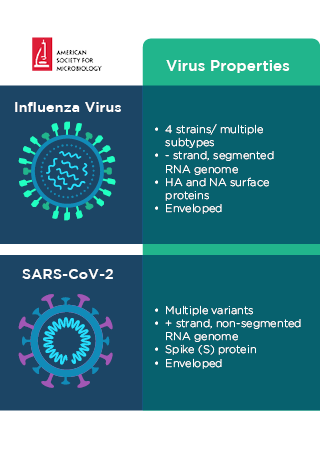
Comparison of influenza virus and SARS-CoV-2 virus properties.
Source: American Society for Microbiology
Genome
Coronaviruses and influenza viruses are both enveloped, single-stranded RNA viruses, and both are encapsidated by nucleoprotein. However, the genomes of these 2 viruses differ in polarity and segmentation. Influenza virus is comprised of 8 single-stranded, negative-sense, viral RNA segments. SARS-CoV-2 has single-stranded, non-segmented, positive-sense, viral RNA.
Surface Proteins
Both viruses possess distinguishing surface proteins that serve as important virulence factors for infection. SARS-CoV-2 is covered in spike (S) proteins that facilitate invasion of host cells. S proteins bind to the host cell receptor, angiotensin-converting enzyme 2 (ACE2), which regulates blood pressure and fluid-salt balances and is expressed by multiple organ systems throughout the body, including the lungs, heart, kidneys, liver, intestines, brain and adipose tissues. Upon binding, SARS-CoV-2 injects its RNA into the infected cell and uses host cell machinery to replicate its genome. Newly synthesized virus particles are then released to infect additional host cells.
Influenza viruses rely on the collaborative functions of 2 viral surface proteins, haemagglutinin (HA) and neuraminidase (NA) to enter and exit host cells. The host cell receptor for influenza viruses is sialic acid, a sugar chain that is fairly ubiquitous and attached to surface lipids and proteins of most host cells, as well as soluble proteins. HA preferentially binds to sialic acid on the surface of respiratory epithelial cells, and mediates entry of the virus to host cells. Once inside, influenza virus also releases its RNA to be copied and synthesized into new virus particles. However, as long as HA remains bound to sialic acid on cell surfaces, newly synthesized virus particles are unable to exit the infected cells. NA cleaves sialic acid from the cell surface, which releases HA and allows progeny viruses to exit infected cells and continue spreading.
Viral Protein Function
Influenza
SAR-CoV-2
Entry into host cells
HA
S
Exit from host cells
NA
Not applicable
Strains and Subtypes
Another important difference between SARS-CoV-2 and influenza is that there are multiple variants of SARS-CoV-2 and 4 different strains (A, B, C and D), and many different subtypes, of influenza virus. SARS-CoV-2 variants are classified as variants under monitoring (VUM) variants of interest (VOI) and variants of concern (VOC). In Oct. 2021, the highly transmissible Delta variant became the dominant circulating variant in the U.S., and by Feb. 2022, Omicron had outcompeted Delta, accounting for >98% of all viral sequences shared on GISAID. Previously circulating VOCs such as Alpha, Beta and Gamma are either no longer detected or are circulating at such low levels that they do not pose a significant, imminent threat to public health.
The 2 most important strains of influenza virus, when it comes to human disease, are influenza A and influenza B, which both cause annual seasonal flu outbreaks. Influenza A virus is further divided into subtypes based on its HA and NA surface proteins. There are 18 possible HA subtypes and 11 NA subtypes, which means 198 combinations are possible. However, only 131 subtypes have been detected in nature, to date.
Viral Evolution and Pandemic Probability
SARS-CoV-2 is a novel virus, which means that we had no available treatments or immunity to the pathogen when it emerged in late 2019. Because of this, the virus was able to spread, unrestrained from host to host, and it didn’t take long for the SARS-CoV-2 outbreak to become a pandemic. Although we have since developed vaccines that are remarkably effective at preventing severe disease and hospitalization from SARS-CoV-2 infection, studies have demonstrated that the spike proteins of seasonal (endemic) human coronaviruses undergo adaptive evolution that is consistent with selection for antibody escape. It is therefore not surprising that SARS-CoV-2 continues to mutate, and the emergence of new variants with S protein mutations that cause increased transmissibility and/or pathogenesis suggest that the novel coronavirus is undergoing selective evolution at the population level.
Importantly, vaccines remain protective against even the most transmissible SARS-CoV-2 variants, including Omicron. However, increasing vaccination while simultaneously decreasing case numbers is the one-two punch that will ultimately be required to slow the spread of this virus, and diligent monitoring of SARS-CoV-2 mutations is key to informing mitigation strategies.
Even though the flu is not a new pathogen, influenza virus is constantly evolving and experiencing varying levels of antigenic drift (and shift) that can make it less recognizable to our immune systems. This has made the development of a universally effective flu vaccine particularly challenging and explains the constant underlying threat that new zoonotic influenza strains might emerge and become pandemic. All cases of pandemic flu in the U.S. have been caused by zoonotic subtypes of influenza A, including the Flu of 1918 (H1N1), the 2005 Avian flu (H5N1) and the 2009 Swine flu (H1N1).
Coinfection Dynamics
We know that coinfection with multiple respiratory viruses is possible. More specifically, coinfection has been reported for SARS-CoV-2 and respiratory syncytial virus (RSV), rhinovirus, other Coronaviridae and the flu. A study published in the Journal of Medical Virology showed that coinfection of SARS-CoV-2 and influenza virus was common during the initial COVID-19 outbreak in Wuhan, China, and patients who experienced coinfection had a higher risk of poor health outcomes.
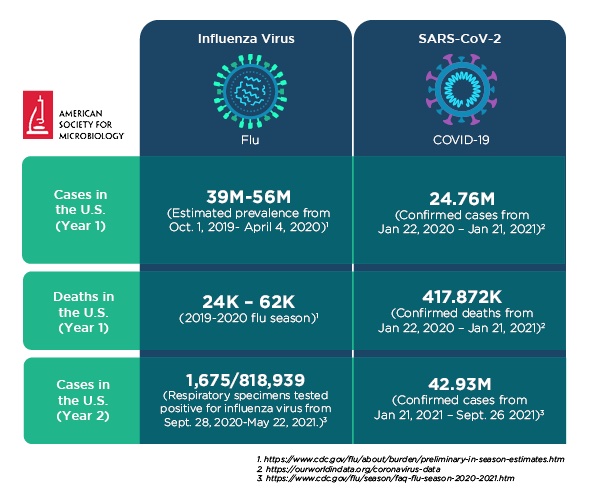
However, the reported incidence of seasonal influenza was uncharacteristically low in both the northern and southern hemispheres during the 2020-2021 Flu season. From September 28, 2020-May 22, 2021 in the U.S., only 1,675 (0.2%) of 818,939 laboratory tested respiratory specimens were positive for influenza virus. Early reports from the southern hemisphere hinted that the season had kicked off mildly. As of July 20, 2020, no region had reported more than 10% test positivity, and several regions, including Southeast Asia and parts of South America and Africa reported 0 cases of the flu. In contrast, in July 2019, most regions in the southern hemisphere were reporting greater than 10% test positivity for seasonal influenza, with the most heavily hit areas reporting greater than 30% test positivity, and an estimated 39-56 million cases of influenza occurred in the U.S. between Oct. 1, 2019-April 4, 2020.
A number of factors likely contributed to the reduction in flu cases during the early years of the pandemic. Non-pharmaceutical interventions (NPIs), such as social distancing, international travel bans, masking and improved hand hygiene, were all used to slow transmission of SARS-CoV-2. Undoubtedly, these NPIs reduced influenza transmission as well, and the fact that, despite these mitigation strategies, COVID-19 continued to spread more prevalently than the flu indicated that SARS-CoV-2 is more contagious than influenza virus. Additionally, according to the CDC, a record number of people elected to receive the flu vaccine during the 2020-2021 flu season. As of Feb. 26, 2021, 193.8 million doses had been distributed in the U.S. It is also possible that insufficient testing and reporting resulting from supply and personnel shortages, as well as pandemic preoccupation, caused case numbers to appear lower than was fully representative of true prevalence.
Overall, it is not completely certain which of these factors had the greatest impact, or how the very low numbers will impact this year’s flu season. Some scientists have postulated that lack of exposure to the flu in recent years could decrease herd immunity and increase host susceptibility to the virus. In fact, from April-Oct. 2022, Australia reported the worst flu season it has seen in 5 years, and many are speculating that the increase in flu in the southern hemisphere will be a harbinger of similar trends in the northern hemisphere in the coming months.
In the event that these 2 viruses do come in contact with one another simultaneously in the same host, it is of great interest whether either pathogen causes viral interference (competitively suppresses replication of the other virus). Because SARS-CoV-2 and influenza virus both infect cells of the respiratory tract, they might have to compete for resources (including cells to infect) during coinfection. As previously noted, the host cell receptors are unique for each of these viruses. Sialic acid is more prevalent than ACE2, but the binding affinity of S protein to ACE2 is remarkably strong. It is possible, but remains uncertain, whether either of these factors contributes a competitive advantage.
The host immune response presents another variable worth considering. Does a host’s immune response to one virus make it more difficult for the other to cause infection? Or is an already immunocompromised host left more vulnerable to secondary infection? Only time and experience will tell. But taking a closer look at disease characteristics can help inform diagnosis and treatment plans as we move forward.
Comparison of COVID-19 and the flu case numbers. Updated Oct. 7, 2021.
Source: American Society for Microbiology
Transmission
The flu and COVID-19 are both primarily spread via small, virus-laced particles called respiratory droplets that are released when an infected person coughs, sneezes, talks or simply exhales. Someone who is nearby may inhale these droplets or become infected through physical contact, like handshaking or hugging, followed by touching their own nose or mouth.
Importantly, individuals do not need to exhibit symptoms to be contagious. Both COVID-19 and the flu can be transmitted by presymptomatic, asymptomatic and mildly symptomatic individuals.
Influenza virus can remain infectious on surfaces outside of the body for up to 48 hours, which means that it’s possible to get sick by touching an object or surface that has recently been coughed on, sneezed on or touched by someone who has the flu. There is evidence suggesting that SARS-CoV-2 RNA may remain present on objects and surfaces for extended periods of time, but how long the virus remains infectious outside of the body has yet to be definitively determined.
Vulnerable populations and age groups are more susceptible to both SARS-CoV-2 and influenza virus, but COVID-19 has shown more superspreading activity than the flu (defined as an instance in which an individual has at least 8 transmissions of the disease to other people).
Flu season occurs in the fall and winter. In the U.S., that means October-March, and in the southern hemisphere, June-September. Although the reason for this seasonality is not entirely understood, influenza virus has been shown to survive longer at low temperatures and low humidity. Other suggested explanations include weakened host immunity, due to decreased sunlight and vitamin D, and increased exposure to the virus, due to indoor cohabitation in the winter. It is still not entirely clear to what extent SARS-CoV-2 exhibits flu-like seasonality and temperature sensitivity. But the persistence of COVID-19 cases throughout the summer has reminded us that these are, indeed, 2 separate viruses.
Fortunately, both SARS-CoV-2 and influenza virus are sensitive to alcohol-based sanitizers and soap, and good hand hygiene is an effective way to reduce transmission.
Incubation
The incubation period for the flu is typically 1-4 days after infection, but the incubation period for COVID-19 is considerably more variable. Most people develop symptoms within 5 days of exposure, however incubation periods of as little as 2 days and up to 14 days or more have been reported.
Symptoms
Respiratory viruses primarily infect cells of the lungs and respiratory tract. As a result, symptoms and modes of transmission are tightly linked to respiration processes. Both SARS-CoV-2 and influenza cause fever, cough, shortness of breath, fatigue, sore throat, runny nose, body aches, vomiting and diarrhea. SARS-CoV-2 also causes loss of taste or smell, and additional, less common, COVID-19 symptoms and complications are continuing to be observed, reported and evaluated.
In serious cases, both the flu and COVID-19 cause pneumonia, respiratory failure, acute respiratory distress syndrome, sepsis, heart attack or stroke, multiple organ failure, severe inflammation and even death.
While most respiratory viruses, including RSV, adenovirus and parainfluenzavirus, exhibit some symptom overlap, that does not mean that the disease progression, severity or pathogenesis of each virus is the same. Symptoms of the flu typically resolve within 5-7 days of onset, but it takes longer to recover from COVID-19 (about 2 weeks for mild cases and up to 6 weeks or more for severe cases).
Diagnosis
Because COVID-19 and the flu present very similarly, they are nearly impossible to differentiate based on symptoms alone. Accurate diagnosis requires laboratory testing to identify genetic or molecular components of the infecting virus.
There are a number of Food and Drug Administration (FDA)-approved diagnostic tests available for the flu, including viral culture, serology, rapid antigen testing, molecular tests and immunofluorescence assays. And the FDA has issued Emergency Use Authorizations (EUAs) for molecular tests, serology assays and rapid antigen testing to diagnose COVID-19 (note that EUAs do not confer FDA approval).
Treatment & Prevention
Remdesivir (VEKLURY®), an antiviral drug that targets RNA-dependent RNA polymerase, the enzyme responsible for replicating the SARS-CoV-2 genome, has received FDA approval for the treatment of COVID-19. Merek's oral antiviral LAGEVRIO (molnupiravir) and Pfizer's oral antiviral PAXLOVID have both received EUA for the treatment of mild-to-moderate COVID-19 in adults (molnupiravir) and adults and children 12+ years of age and weighing at least 88 lbs (PAXLOVID). Other candidate drugs are being tested and developed, but the most effective way to prevent severe COVID-19 remains through vaccination. Finally, supportive care continues to be a critical component of disease management.
A number of antiviral medications may be prescribed to treat influenza, including NA inhibitors such as oseltamivir (Tamiflu), zanamivir (Relenza) or peramivir (Rapivab), and a polymerase acidic endonuclease inhibitor, baloxavir (Xofluza). All of these medications inhibit, but do not completely eliminate, influenza virus. An annual seasonal flu vaccine is the best way to protect against the flu.
As we move through the winter, the best things we can do to prepare for the coinciding flu season and global COVID-19 pandemic are get vaccinated against COVID-19 and the flu and practice good hand hygiene and social distancing measures.

 Source: American Society for Microbiology
Source: American Society for Microbiology
